Is your patient hooked on Vicodin? Try this
The Carlat Psychiatry Blog, Volume , Number ,
https://www.thecarlatreport.com///

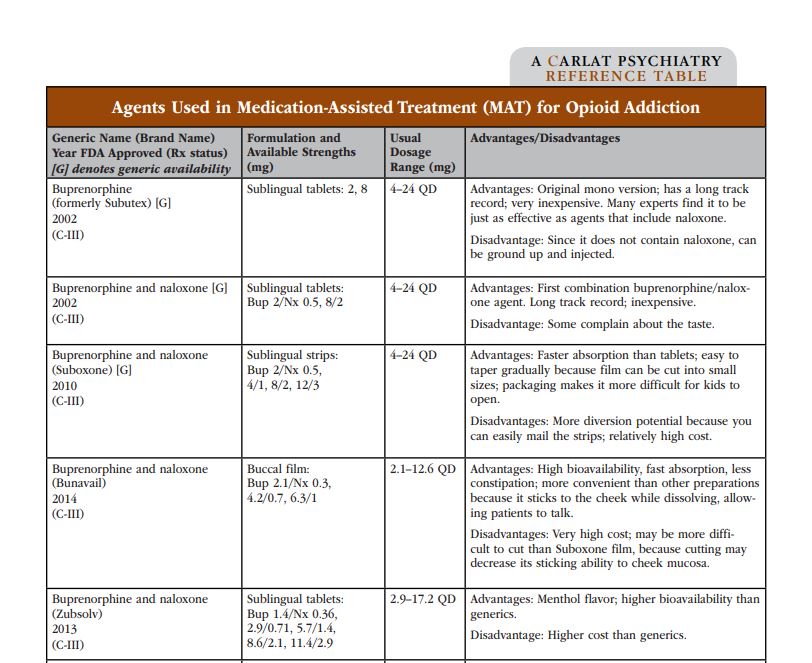
I don’t specialize in addiction treatment, but occasionally I do have patients who tell me they’ve been overusing prescription narcotics. For example, I once treated a woman for depression who was dependent on Vicodin that was originally prescribed after surgery by her OB/GYN. Over the years she had tried quitting on her own, unsuccessfully. Her PCP had continued to prescribe it as long as she didn’t increase the dose. She asked me for help, and I referred her to a local addiction treatment program, but she declined to go because she didn’t view herself as an “addict.” I didn’t feel qualified to manage a detox, so I continued to encourage her to see an addiction specialist. Eventually, she left my practice because of a move. I wish I had read Dr. Michael Weaver’s article in the upcoming issue of The Carlat Addiction Treatment Report, which explains, in very practical terms, how to treat patients with different levels of severity of opiate abuse. Here’s a sample reference table covering methadone and other medications used to treat opioid addiction: If you aren’t subscribed to The Carlat Addiction Treatment Report, I urge you to give it a try. You’ll have instant access to all of the articles we’ve written about opioids. Not only will you learn the latest unbiased information about addiction treatment, but you’ll earn CMEs while you’re doing it. All with our usual 100% money back guarantee if the newsletter does not turn out to be extremely useful for your practice.